
What Happens Between Therapy Sessions — and Why It Matters More Than You Think
Introduction
Therapists often do their most important work in a setting that only captures a fraction of a patient’s lived reality. One session may reveal a concern, a breakthrough, or a risk signal, but it cannot show what unfolds in the hours and days after the patient leaves the room. That missing time is not a side note; it is where many of the most meaningful changes, setbacks, and coping decisions actually happen (Kazantzis & Miller, 2022; Bennion et al., 2024).
For clinicians, this creates a fundamental challenge: therapy is observed in snapshots, while distress and recovery unfold continuously. Research on between-session homework, ecological momentary assessment, and session frequency all points to the same reality — what happens outside the appointment often determines whether therapeutic insight becomes durable change (Bennion et al., 2024; Shiffman et al., 2008; Erekson et al., 2015).

The “Between Sessions” Reality
The period between appointments is where patients face the actual conditions that shape symptoms and behavior: conflict at home, workplace stress, sleep disruption, substance use triggers, shame spirals, avoidance, social support, and moments of effort that never make it into the note. In this space, patients practice coping skills, interpret setbacks, and decide whether to reach out, withdraw, or continue the work they started in session (Bennion et al., 2024; WHO, 2025).
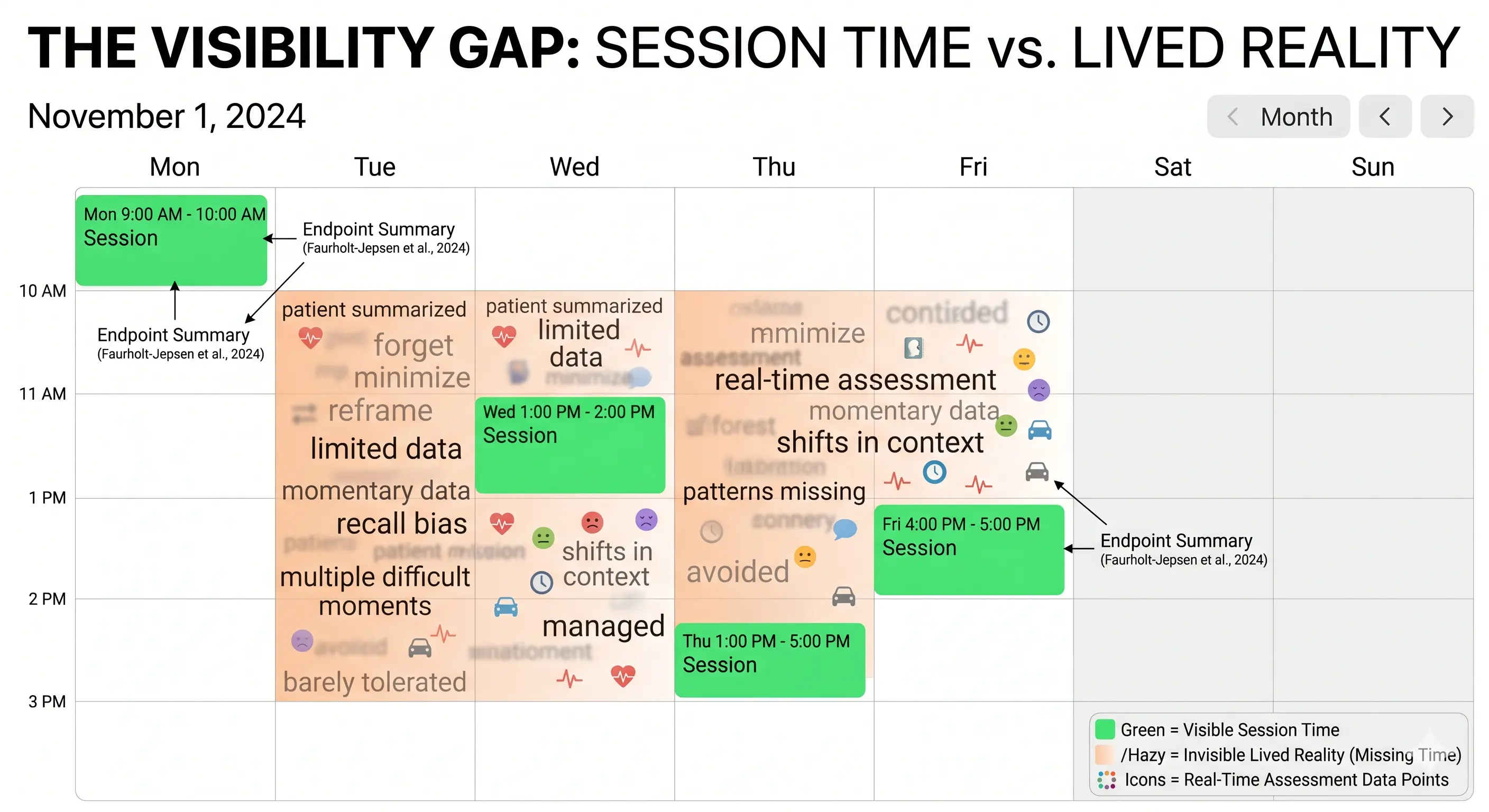
This is also where emotions tend to fluctuate in ways that are easy to miss in a retrospective conversation. Ecological momentary assessment research shows that repeated, real-time sampling can capture context, mood shifts, and behavioral patterns that retrospective recall often blurs or omits (Shiffman et al., 2008; Faurholt-Jepsen et al., 2024). In other words, the “between” is not downtime; it is the clinical terrain.
Why This Time Is Critical
Behavior change does not occur in a vacuum. It happens in the same environments where people face cues, constraints, relationships, and routines, which is why behavioral science emphasizes mechanisms and context rather than isolated intentions (NIH, 2018; NIH, 2023). A patient may fully understand a skill in session and still struggle to use it when the phone buzzes, the child melts down, or the old coping pattern feels easier in the moment.
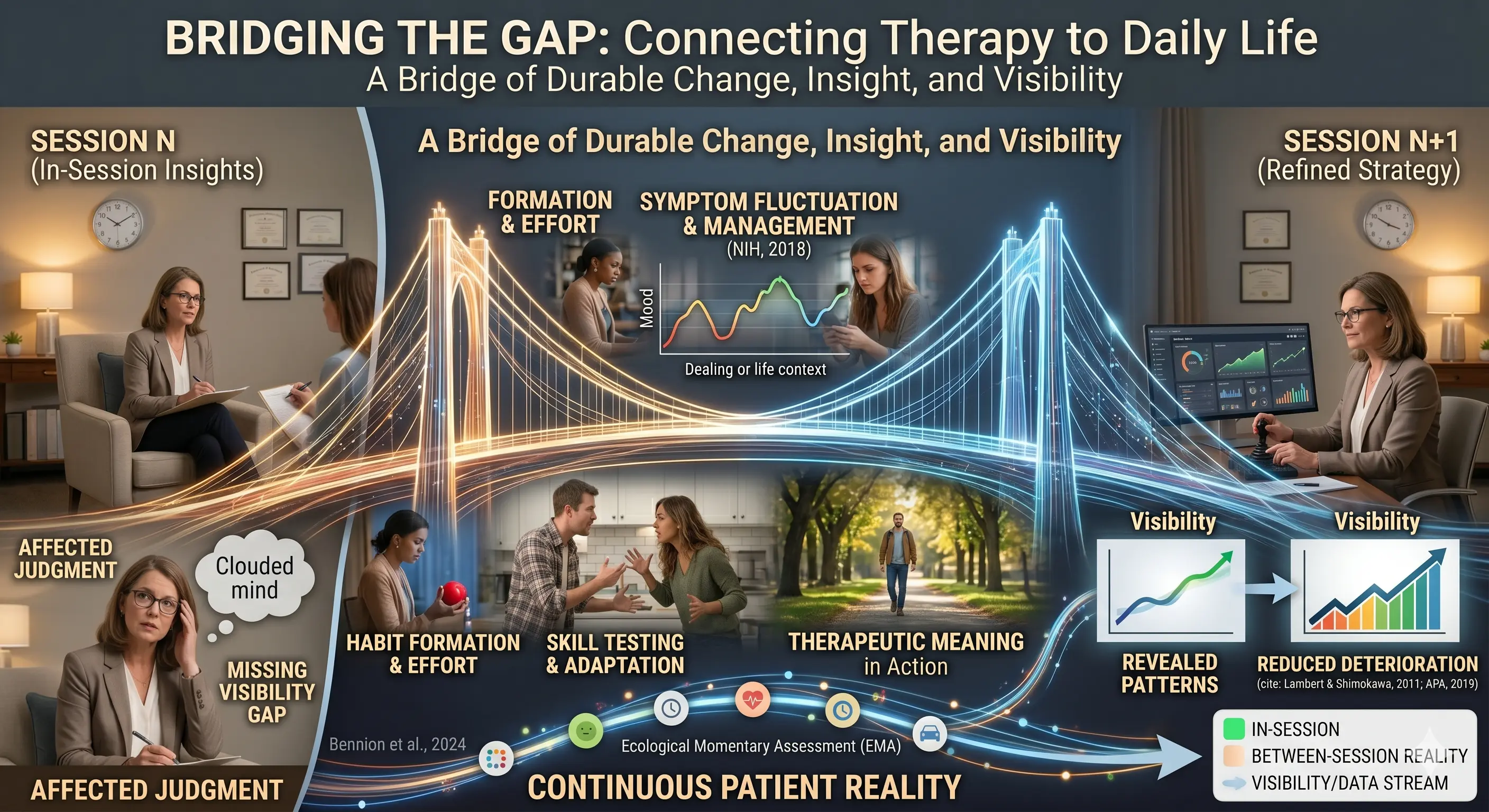
That is also why the therapy hour can be misleading if it is treated as the full picture. Between-session activities — whether they are reflections, exposures, behavioral experiments, or simple tracking — are designed to transfer insight into real life, where generalization is tested and reinforced (Bennion et al., 2024; Kazantzis & Miller, 2022). Sessions are the laboratory; life is the field.
The Visibility Gap
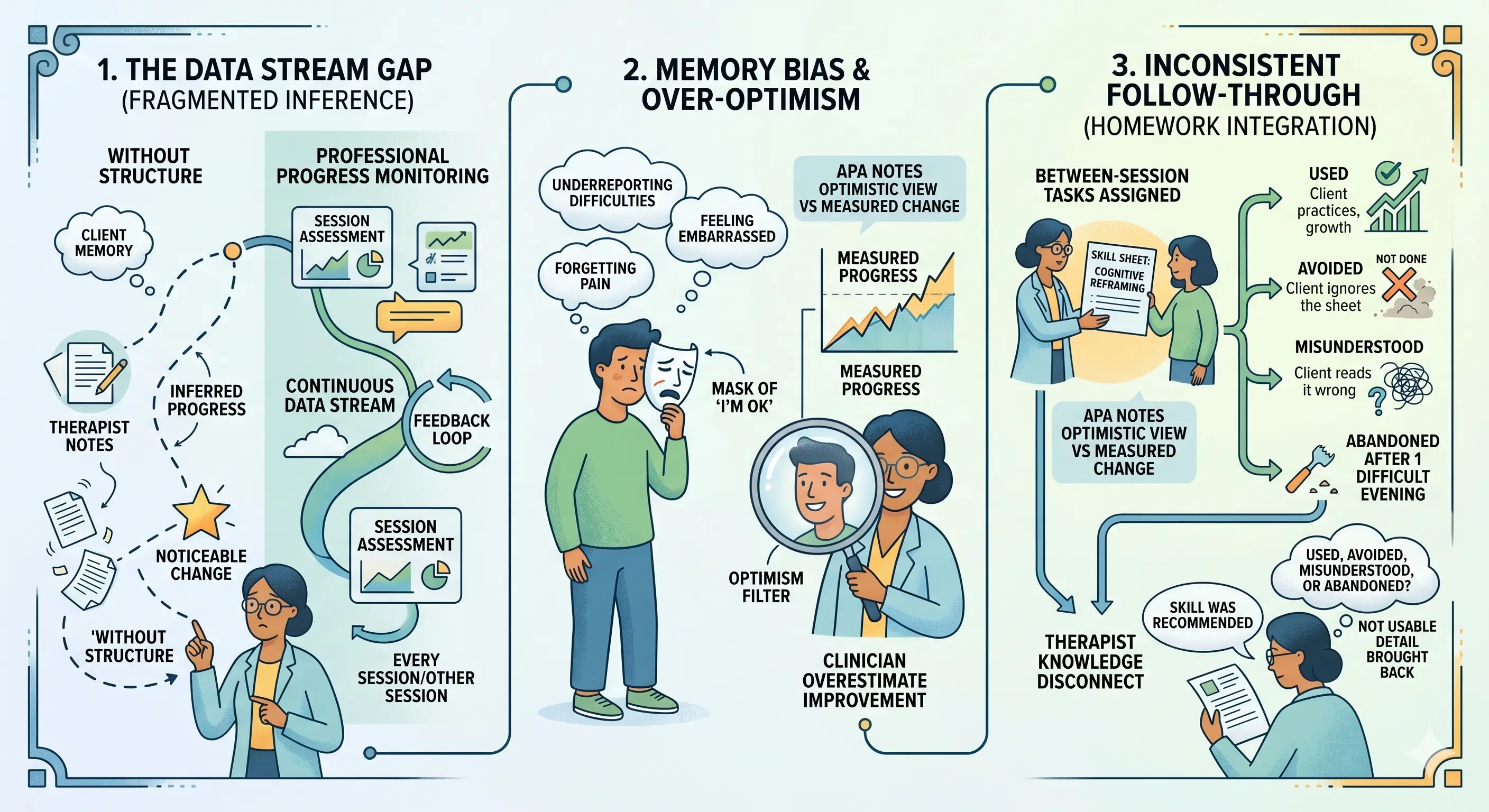
Clinicians usually rely on memory, session notes, and patient recall to understand what happened between appointments. Those sources are useful, but they are inherently filtered: patients summarize, forget, minimize, or reframe; clinicians infer patterns from limited data; and notes often preserve conclusions more than lived experience. That creates a visibility gap between what is said in session and what actually occurred during the week.
The risk is not only missed information, but distorted information. Real-time assessment research shows that momentary data can reduce recall bias and reveal patterns that endpoint summaries miss, including shifts tied to time, place, and social context (Shiffman et al., 2008; Faurholt-Jepsen et al., 2024). In practical terms, a patient’s verbal “I was fine” may coexist with multiple difficult moments that were managed, avoided, or barely tolerated.
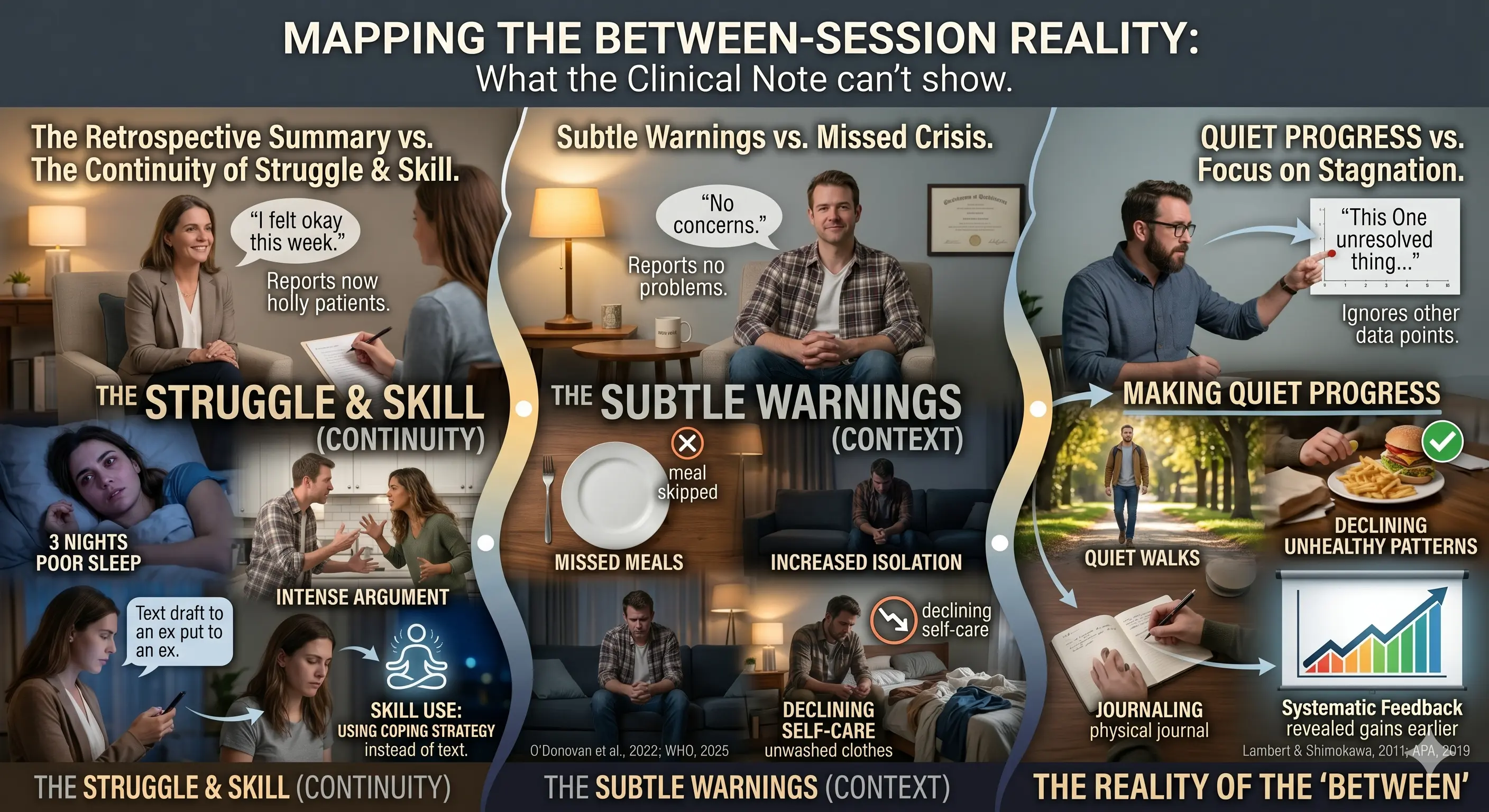
Real-World Scenarios
A patient says, “I felt okay this week,” and the session ends there. But between appointments they had three nights of poor sleep, one intense argument, and an evening when they nearly texted an ex-partner before using a coping strategy instead. The session captures the summary, not the struggle or the skill use.
Another patient reports no major concerns, yet subtle warning signs were present all week: missed meals, increased isolation, and declining self-care. Because those changes were spread across days, they did not present as an obvious crisis in the room. Continuity-of-care literature consistently notes that early intervention matters because problems are easier to address before they escalate (O’Donovan et al., 2022; WHO, 2025).
A third patient is making quiet progress that never gets documented. They are going on walks, using journaling, and declining one unhealthy pattern after another, but in session they focus on the one thing that still feels unresolved. Without better visibility, clinicians can underestimate gains and overestimate stagnation. Progress monitoring research suggests that systematic feedback can improve responsiveness and reduce deterioration when clinicians can see change earlier (Lambert & Shimokawa, 2011; APA, 2019).

The Limits of Traditional Approaches
Traditional documentation is important, but it was never built to capture continuous reality. Notes usually reflect what was discussed, not the full sequence of triggers, responses, and recovery attempts between visits. Occasional check-ins help, but they still produce intermittent data, which means the most intense moments may happen just before or after the contact window.
Verbal summaries also depend on the patient’s ability to remember, organize, and disclose. That is especially limiting when symptoms fluctuate, avoidance is high, or shame makes certain events hard to name. Because session frequency itself can influence how quickly change is detected, longer gaps may slow recognition of both improvement and deterioration (Erekson et al., 2015).
Impact on Care and Outcomes
When clinicians cannot see the between-session period, interventions may arrive too late. Small regressions can become larger problems before they are discussed, and positive momentum can go unrecognized until it has already been lost. That creates uncertainty in formulation, risk assessment, and treatment pacing.
The broader outcome is less precise care. Without reliable visibility into real-world functioning, it becomes harder to distinguish nonresponse from partial response, adherence problems from environmental barriers, and genuine stabilization from temporary relief. Monitoring research suggests that feedback and progress tracking can improve outcomes by helping clinicians respond session by session rather than relying on impression alone (Lambert & Shimokawa, 2011; APA, 2019).
What Better Visibility Would Look Like
Better visibility would be consistent, low-friction, and grounded in real life rather than isolated recall. It would help clinicians understand patterns as they emerge, not only after they harden into a crisis or a retrospective story. It would also make it easier to notice the small, clinically meaningful changes that patients often forget to mention.
It would support real-time awareness of emotional shifts, behavior patterns, triggers, and coping attempts. It would also make pattern recognition easier across weeks, not just within one appointment, which is especially valuable in conditions marked by rapid fluctuation or context sensitivity (Shiffman et al., 2008; Faurholt-Jepsen et al., 2024). Just as important, it would be easy enough for patients to use during ordinary life, not only during high-motivation moments.
Conclusion
The space between therapy sessions is not empty time. It is where habits form, symptoms intensify or ease, skills are tested, and the meaning of therapy becomes visible in daily life (Bennion et al., 2024; NIH, 2018). When clinicians only see the appointment itself, they risk missing the very period where change is most likely to happen.
For therapists, psychologists, counsellors, and social workers, that gap is more than an inconvenience. It affects judgment, timing, and confidence in care. The profession has spent decades refining what happens in session; the next step is taking the invisible time between sessions just as seriously.
References
- American Psychological Association. (2019). Need help tracking patient outcomes?
- Bennion, M., et al. (2024). Between-Session Homework in Clinical Training and Practice.
- Erekson, D. M., et al. (2015). The relationship between session frequency and psychotherapy outcomes.
- Faurholt-Jepsen, M., et al. (2024). Mobile-based ecological momentary assessment and mental health symptom dynamics.
- Kazantzis, N., & Miller, I. W. (2022). Between-session homework and processes of change.
- Lambert, M. J., & Shimokawa, K. (2011). Patient feedback systems and psychotherapy outcomes.
- National Institutes of Health. (2018). The NIH Science of Behavior Change Program.
- National Institutes of Health. (2023). Behavior Modification for Lifestyle Improvement.
- O’Donovan, A., et al. (2022). Continuity of care and therapeutic relationships as critical factors.
- Shiffman, S., Stone, A. A., & Hufford, M. R. (2008). Ecological momentary assessment.
- World Health Organization. (2025). Community-based mental health care and continuity of care.