
Introduction
Therapy often looks structured on the calendar and incomplete in real life. A client may have 50 minutes in the room, but most of the week happens outside it—during arguments, commutes, sleepless nights, panic spikes, avoidance, and small moments of coping that never make it into the next session. That creates a visibility gap: clinicians must make decisions about progress using fragments rather than a continuous view of what is actually happening [CPA Task Force, 2018][APA, 2019].
That gap matters because psychotherapy is not just about what a person says on Tuesday afternoon. It is about whether the change holds on Wednesday night, whether a coping strategy was used during a conflict on Friday, and whether symptoms quietly worsened after a missed appointment or a stressful event. Routine progress monitoring was developed to address exactly this problem, but research and professional guidance show that it is still unevenly used and often difficult to implement well [CPA Task Force, 2018][Lambert et al., 2018][NICE, 2011].
The Reality of Therapy Workflows
Most clinicians are not missing progress because they do not care. They are missing it because the workflow is compressed, interrupted, and cognitively demanding. In a typical session, a therapist must listen for content, observe affect, manage alliance, track risk, keep the treatment plan in mind, and make enough mental space to document what matters afterward. APA materials on measurement-based care emphasize that repeated patient-reported outcomes can improve decision-making precisely because memory and intuition alone are not reliable enough for this task [APA, 2019][APA, 2023].
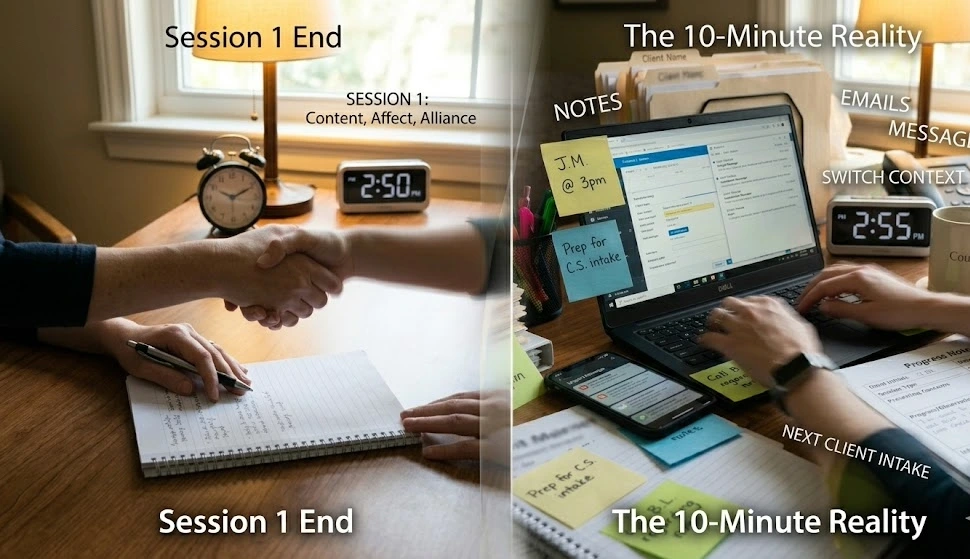
Between sessions, the work becomes even less visible. Therapists may be seeing multiple clients in succession, writing notes, responding to urgent messages, consulting supervisors, and switching repeatedly between different clinical contexts. That context switching increases the chance that subtle patterns are not noticed: a slight drop in hopefulness, a new avoidance behavior, a homework pattern that has disappeared, or a recurring trigger that only shows up once every few weeks. By the time the next session arrives, the week’s most important evidence is often already filtered through memory and a brief note.
Why Progress Is Hard to Track
The first problem is simple: there is no continuous data stream in most therapy relationships. Progress is often inferred from what clients remember, what therapists notice, and what is recorded in notes, rather than from a regular and standardized view of change. Professional sources define progress monitoring as repeated assessment, often every session or every other session, with feedback that helps therapists respond session by session [CPA Task Force, 2018][McGill Psychology, 2020]. Without that structure, progress becomes easy to misread.
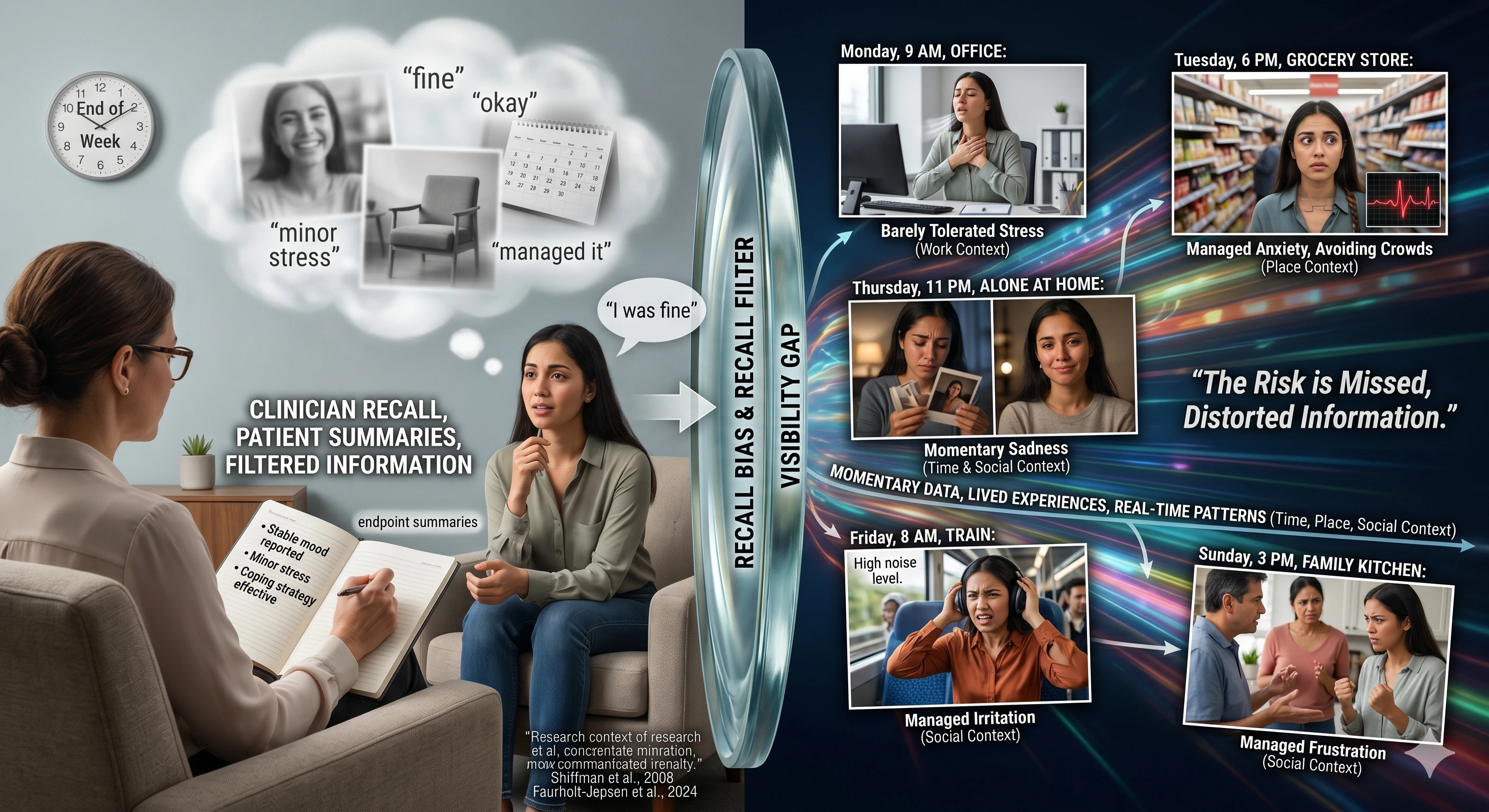
A second problem is memory bias. Patients may underreport difficult moments because they want to appear okay, feel embarrassed, or genuinely forget the most painful parts of the week by the time they sit down in the office. Therapists can also overestimate improvement, especially when a client is articulate, engaged, and pleasant to work with. APA notes that clinicians often hold overly optimistic views of treatment progress compared with measured change [APA, 2019]. That is not a character flaw; it is a predictable feature of human judgment under uncertainty.
A third problem is inconsistent follow-through. Even when between-session tasks are assigned, clients do not always complete them in the way intended, or they complete them but do not bring back usable detail. Research on between-session homework shows that its value depends on how it is integrated, monitored, and discussed, not merely assigned [Kazantzis et al., 2024]. In practice, that means the therapist may know a skill was recommended, but not whether it was used, avoided, misunderstood, or abandoned after one difficult evening.
The Limits of Current Methods
The most common tools—clinical notes, recall, and occasional check-ins—were never designed to provide a granular picture of change. Notes are indispensable for continuity, ethics, and billing, but they are retrospective summaries, not live tracking systems. They capture the story a therapist can reconstruct after the session, which is often different from the story that unfolded in real time.
Recall is even more limited. A client may describe the “average” week while forgetting the worst 20 minutes that actually reveal a relapse pattern. A therapist may remember the session that felt emotionally significant and miss the quieter shift that predicted deterioration. NICE has acknowledged the potential value of routine outcome measurement because feedback can prompt earlier interventions, but it also highlights that implementation frequency and burden remain important considerations [NICE, 2011]. That caution reflects a real tension: the method is useful, but the field still struggles to make it workable at scale.
Occasional check-ins help, but they create a false sense of visibility. A therapist might ask, “How has the week been?” and receive a reassuring answer that misses the details most relevant to treatment. The problem is not that clients are dishonest or therapists are inattentive. It is that one conversation a week cannot reliably capture the complexity of lived experience between those conversations. Measurement-based care exists because the gap is structural, not merely interpersonal [APA, 2023].

Real-World Examples
Scenario 1: Underreported decline
A client with depression says the week was “fine” because they showed up, got through work, and did not have a crisis. On closer questioning, it turns out they spent two evenings in bed, skipped meals, and stopped answering messages from friends. The therapist may not catch this pattern until symptoms have already deepened, because the client’s summary sounded stable and the most concerning behaviors were experienced as normal coping, not as warning signs.
Scenario 2: Improvement that hides avoidance
A client with panic disorder reports less anxiety overall, and the therapist sees genuine progress in session. But the client has quietly begun avoiding the train, the gym, and social plans because they fear panic in public. The person feels safer in the short term, so self-report can sound positive even while functioning is narrowing. Without repeated measurement or a consistent way to ask about avoidance, the therapist may miss that improvement in distress is coexisting with worsening impairment [Lambert et al., 2018].
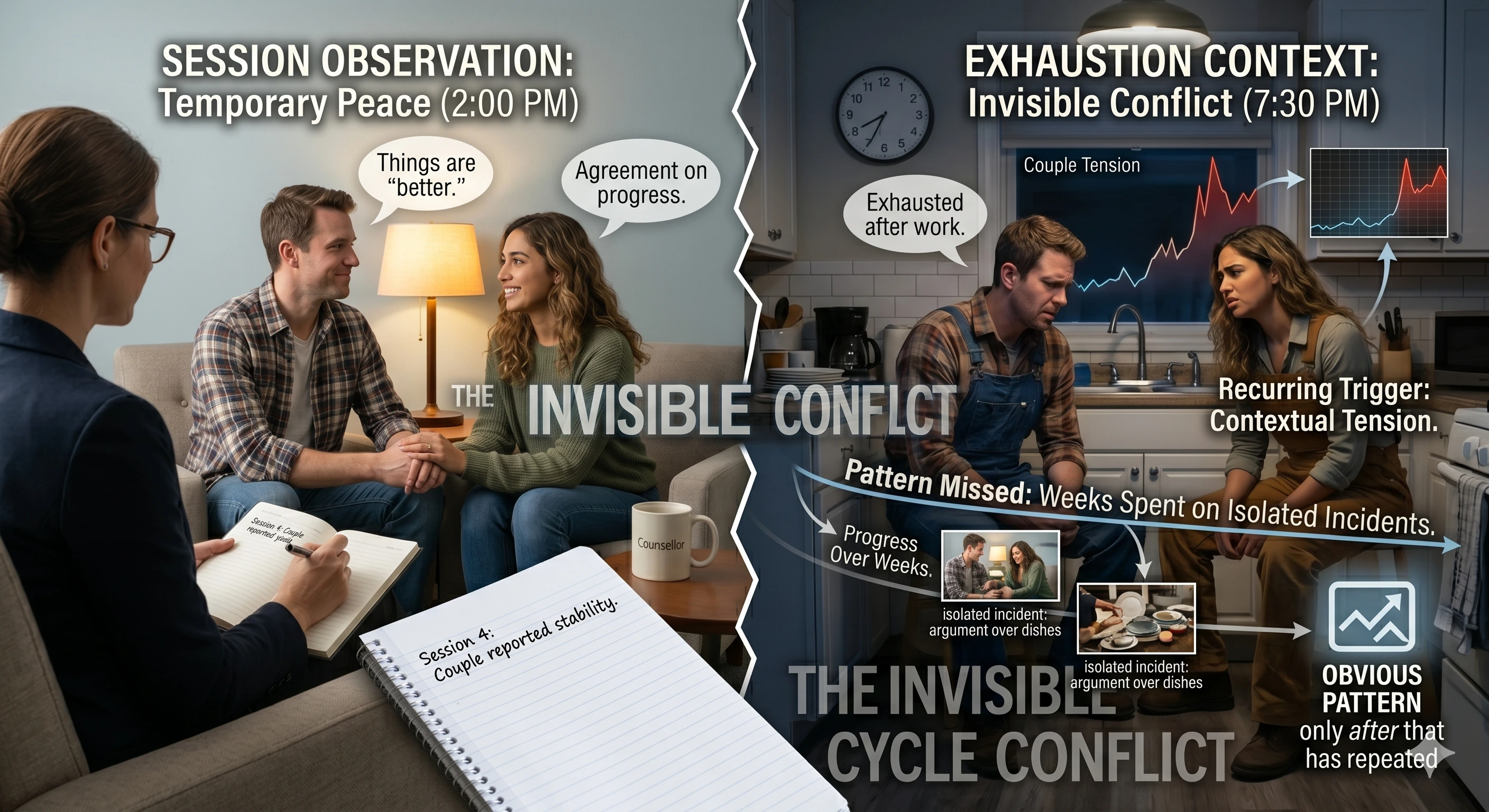
Scenario 3: Patterns missed in context
A couple in therapy agrees that things are “better,” yet the tension that drives conflict only appears when both partners are exhausted after work. Because the clash is context-dependent, it does not show up in every session. By the time the pattern becomes obvious, the therapist has already spent several weeks responding to isolated incidents rather than the recurring trigger. This is where between-session visibility matters most: it can reveal whether progress is durable or just temporarily easier to describe in the office.
The Impact on Outcomes
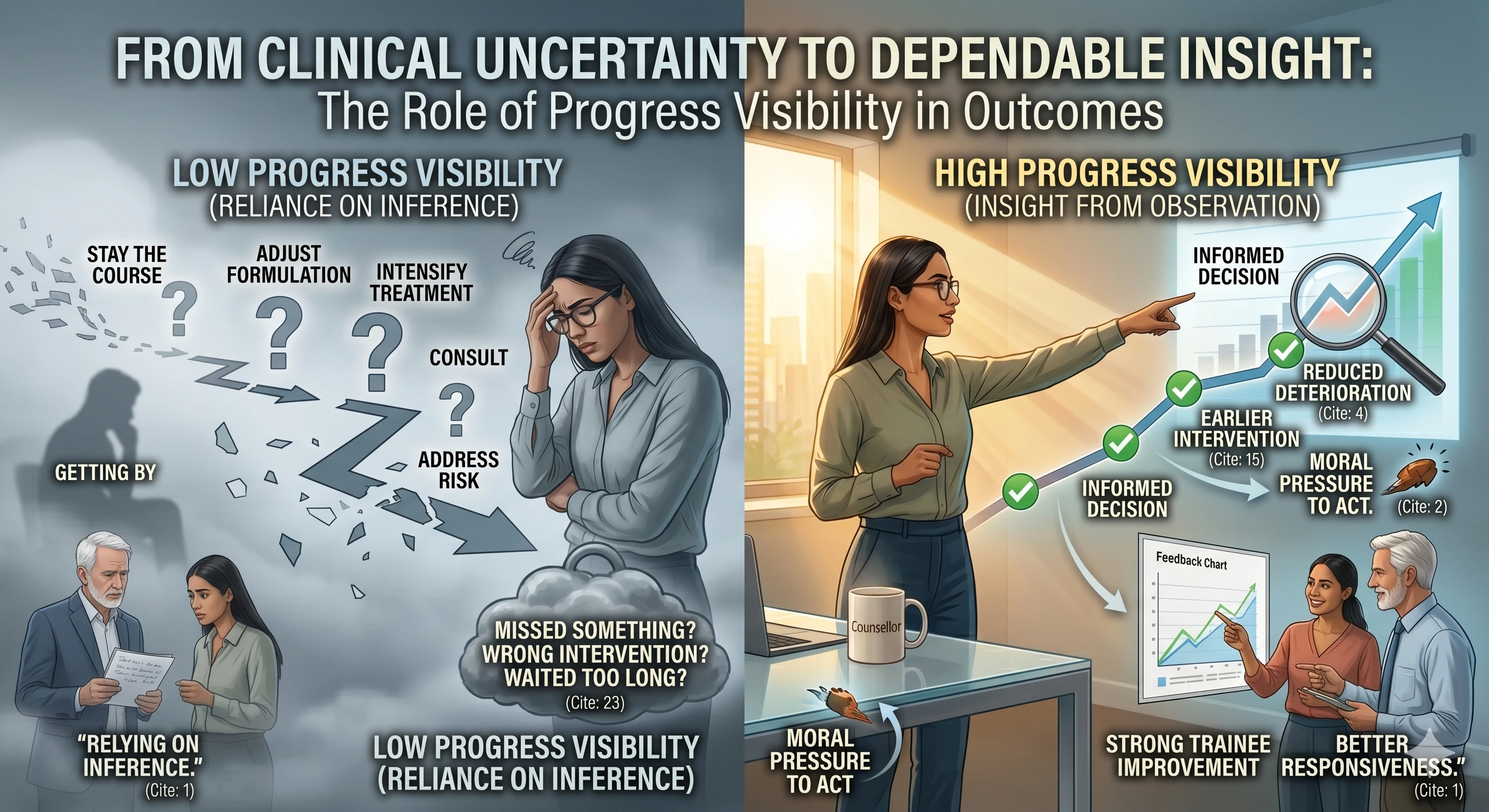
When progress is hard to track, clinical uncertainty rises. Therapists must decide whether to stay the course, adjust the formulation, intensify treatment, consult, or address risk, but the evidence base in front of them is incomplete. Research on routine outcome monitoring and feedback suggests that regular measurement can improve outcomes and reduce deterioration, particularly for clients at risk of treatment failure [Lambert et al., 2018][de Jong et al., 2024]. The implication is straightforward: when the field has better visibility, it can intervene sooner.
The emotional burden is real as well. Therapists often carry the discomfort of not knowing whether the work is helping between visits. That uncertainty can lead to second-guessing, over-reliance on intuition, or the feeling that a client is “getting by” without truly progressing. It also creates a moral pressure: when a case stalls, clinicians may wonder whether they missed something, chose the wrong intervention, or waited too long to adjust course [Hayes et al., 2025].
There is also a supervision and training impact. Feedback systems are associated with stronger trainee improvement and better responsiveness to clients’ needs, which suggests that progress visibility is not just a service-level issue but a clinical skill issue [CPA Task Force, 2018]. Therapists who lack dependable feedback have to rely more heavily on inference, and inference is weaker than observation when the question is whether change is happening outside the room.
What an Ideal Approach Would Require
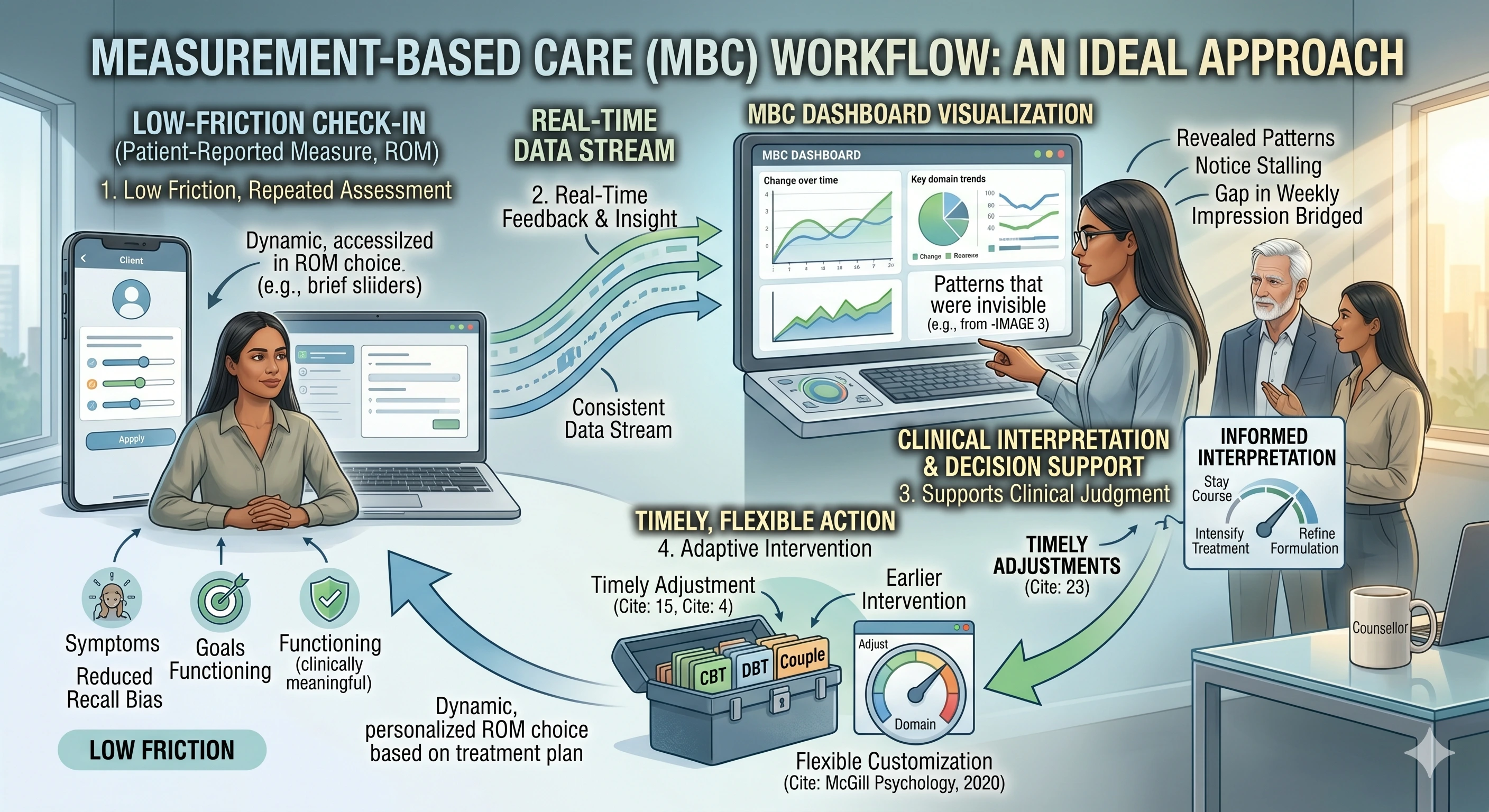
An effective approach would need to be consistent without being burdensome. It would need to provide a clearer picture of change over time, but in a form that fits the actual rhythm of therapy work. Routine outcome monitoring literature and APA guidance both point toward repeated, patient-reported measurement as a core element of better visibility [CPA Task Force, 2018][APA, 2023].
It would also need to be:
- Low friction, so clients can complete it without feeling like they are being tested.
- Objective enough, so progress is not shaped only by memory or rapport.
- Clinically meaningful, so the measures reflect symptoms, functioning, goals, and risk.
- Timely, so the therapist can respond before problems become entrenched.
- Flexible, because different clients need different domains tracked across treatment [McGill Psychology, 2020][NICE, 2011].
Just as importantly, it would need to support interpretation rather than replace it. Data alone does not help if it is too broad, too infrequent, or disconnected from the therapeutic conversation. The best possible system would make it easier to notice what is changing, where change is stalling, and when a weekly impression is no longer enough.
Conclusion
Therapists struggle to track progress between sessions because the real work of therapy happens in the spaces that traditional workflows rarely capture. Notes are retrospective, memory is biased, self-report is incomplete, and a once-a-week conversation cannot reliably reveal the full pattern of improvement, avoidance, relapse, or risk [APA, 2019][Lambert et al., 2018][NICE, 2011]. That is why the challenge is not simply “better documentation.” It is a visibility problem at the heart of outpatient mental health care.
The most important takeaway is not that therapists are failing. It is that the current way of seeing patient change is too sparse for the demands of modern practice. When progress is only partially visible, clinical confidence suffers, interventions come later than they should, and both patient and clinician carry more uncertainty than necessary [CPA Task Force, 2018][Hayes et al., 2025].